Arlo
Arlo is an at-home stroke rehabilitation system that connects clinician-guided care with game-based therapy. Clinicians prescribe daily therapeutic games aligned with a patient’s personal goal, such as making an apple pie. That goal is broken into 3 to 5 milestones like mixing ingredients, placing a pan in the oven, and decorating. Each milestone targets specific movements including arm flexion, grip strength, and finger dexterity. Patients play prescribed games through an app, such as putting groceries away, where they reach, grip, and place objects at varying heights and force levels. A paired physical controller with motion sensors and grip sensors tracks arm movement, orientation, speed, and pressure. Progress data is shared with clinicians to personalize recovery and support measurable, meaningful progress at home.

Timeline
20 weeks,
Fall 2025-Winter 2025
Team
Ann Mulgrew
Tools
Figma
Rhino
Role
Product Designer
Design Researcher
Project Space
People going through a stroke often feel like they aren’t themselves during the recovery process. They feel lost, unmotivated, lonely throughout the recovery process. My thesis explores ways to help survivors feel more engaged and empowered throughout their recovery. I aim to design a product that reduces barriers to rehabilitation by creating something that feels motivating, can be done independently, and supports the improvement of skills.
01 Project Context
WHAT'S A STROKE?
A stroke happens when the blood flow to a part of the brain stops. Without that blood flow, brain cells no longer get the oxygen that they need.
MEET MAYA & HER MONSTER
Maya is a mother of three living her normal life. Then one day, a little monster entered her life. The monster made her feel...








HOW DOES A STROKE IMPACT MAYA'S LIFE?
This “monster” is like a stroke. It enters someone’s life suddenly and alters their very sense of self. When Maya had her stroke, her recovery journey was long and complicated. She wants to move and think better again, but more importantly, she wants to feel like herself again. So how might we help Maya do that?
WHAT'S THE MAIN PROBLEM?
Stroke survivors feel a range of emotions & are affected in many ways. The main thing that they want to get back to is feeling like themselves again.
02 Research
To understand this space, I conducted secondary research, visited a stroke rehabilitation research lab, joined stroke survivor online communities, and interviewed stroke survivors, caregivers, and clinicians.

INTERVIEWS
I’ve done interviews (4 PT/OTs, 3 stroke survivors, 1 caregiver, and 1 medical innovation specialist) and site visits (stroke rehab lab) about the stroke recovery process.


CURRENT STATE RECOVERY JOURNEY MAP OF MAYA'S STROKE RECOVERY
Then I mapped out Maya, Maya's caregiver (David) and the medical staff's actions out to better understand how each of these different users affect and interact with one another throughout the entire journey and better understand where pain points lie and where interventions could be placed.

INSIGHT #1: RECOVERY RUNS ON MOTIVATION
Motivation is the engine of recovery; social support is the upgrade to make that engine run better.
Motivation makes or breaks the recovery process. Clinicians observe that patients with clear, personally meaningful goals (e.g. walking your daughter down the aisle) recover more effectively. These goals provide emotional fuel. Strong social support also plays a major role in the motivation part of recover - without key motivators or consistent support, progress often stalls.
PATHWAYS OF STROKE RECOVERY
I developed frameworks to better understand how the insights, “How Might We” questions, and notes I gathered revealed potential opportunity spaces. I began by identifying the main pathways of stroke recovery. Medical professionals recognize five key types of recovery. However, there is a sixth pathway, one acknowledged by stroke survivors but often overlooked by medical teams. And that is the emotional recovery process.

RECOVERY TYPES
Maya is very well supported when it comes to her PT,OT, and speech therapy but when it comes to her feeling like herself again (so the emotional and behavioral sides of recovery) there's not much that her clinician helps her with since it isn't part of the formal stroke recovery process. That space is largely left unaddressed.

INSIGHT #2: WHO I AM VS WHAT I CAN DO
A stroke survivor’s idea of “success” differs from a clinician’s.
Clinicians often define success as a patient regaining as much ability as possible. From the patient’s point of view, “success” is reclaiming their identity (so adapting to this “new normal” in ways that reflect their “old normal” - who you are vs what you can do).
PATIENT VS CLINICIAN PRIORITIES
A stroke survivor’s definition of success is different from a clinician’s definition of success. For clinicians it's often based on the metrics so all those improvements that the stroke survivor is making that is measurable through numbers. But for stroke survivors it’s most important for them to feel like themselves again. Clinicians really value occupational therapy, physical therapy, and speech therapy. This is also important to patients, but what is most important is the emotional side of things - so finding and feeling like themselves again. There’s a big gap there and an opportunity to fill that in.
INSIGHT #3: CARE ENDS, RECOVERY DOESN’T
Recovery needs exceed what insurance allows. As a result, patients lose guidance once they leave therapy.

Patients and clinicians need more time together, but coverage rarely allows it, leaving patients to navigate recovery largely on their own after discharge. Once patients leave the facility, PTs, OTs, and STs cannot track their progress, even though survivors want clear evidence that their efforts at home are working. Seeing measurable improvement is essential for confidence and motivation.
AT-HOME RECOVERY
When it comes to the at-home recovery, it's really difficult for Maya to understand if she's making improvements physically. So how can we make that progress known to Maya and how we can connect it to her personal goals is what I am trying to explore.
03 Testing
I conducted three rounds of testing throughout this project. The first round focused on concept testing with both clinicians and stroke survivors to validate the overall idea. In the second round, I worked with stroke survivors to explore what specific features would be necessary for the system to support their recovery. And in the final round, I tested with clinicians to understand what features and progress insights they would need in order for this tool to be useful in a rehabilitation setting.
CONCEPT IDEATION: LIGHTNING BRAINSTORMING
In order to prepare for each of my testing sessions, I conducted several rounds of ideation. I noted down a variety of ideas, including some co-created with others. From there, I began identifying which ideas felt the most “sticky”.





CONCEPT IDEATION: JOTTING DOWN IDEAS FOR STIMULI TESTING
Using the narrowed-down ideas, I started developing quick sketches for stimuli testing. I wanted to evaluate these prototypes through conversation and a short set of activities.





TESTING FORMATS
I conducted two rounds of stimuli testing.
-
Round 1: Presented five distinct concept directions developed from an initial ideation phase. Each session began with a brief project recap, followed by a short interview to understand patient and clinician goals. Participants were then guided through a storyboard that extended across all five concepts, allowing me to compare reactions to key variables such as progress tracking, responsibility distribution, and therapy format (e.g., game-based vs. intentional practice). Participants were primarily stroke survivors.
-
Round 2: Similar to round 1, five distinct concepts were presented. Each session began with an overview and short interview. There were two activities. Activity 1 is similar to what was conducted in Round 1 of testing, except with a more clinician-focused lens. Activity 2 took those 5 ideas and extracted key features from each of them. Participants were then asked to mark each feature with a red, yellow, or green dot. Dots signal which features are must haves vs nice to haves vs not needed. Participants were primarily clinicians and researchers.

TESTING SYNTHESIS
I gathered and compared notes from each round of testing. Through synthesizing and analyzing my results, I developed the core features and design requirements of my solution.

DESIGN REQUIREMENTS
04 Design Story
SETTING UP THE SCENE FOR ARLO
To understand how Arlo helps Maya, let’s learn a bit more about her. You’ve already met Maya and know that she had a stroke. She’s a mother of three, and family is everything to her.




But once Maya is back at home, how does she work towards that goal and target areas at home?
That's where Arlo comes in.
05 Arlo
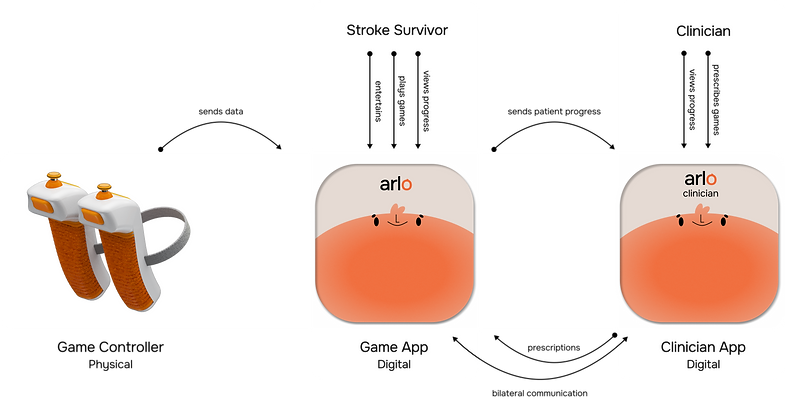
COMPONENTS OF THE SYSTEM
Arlo is a connected rehabilitation system with three components: a clinician-facing app, a stroke survivor app, and a sensor-based game controller. Paulina uses Arlo to prescribe Maya minigames that are aligned with her apple pie goal. As Maya plays, the controllers track grip strength, motion, and mobility in real-time. Arlo then translates that physical data into clear, meaningful progress - especially during the at-home phase where clarity is often missing.
CONTROLLER DIAGRAM
The controller tracks progress through a variety of sensors. Arm Motion & Orientation is measured with an IMU. It detects arm movement direction, speed and acceleration of motion, angular rotation (how the arm is facing). FSRs are used to measure force. These are low cost sensors, flexible sensors that can detect Maya’s grip strength, pressure changes over time, contact force patterns.

Inertial Measurement Unit (IMU)
-
3-axis accelerometer for linear movement
-
3-axis gyroscope for arm & wrist rotation
-
What can be detected: arm movement, direction, speed, acceleration of motion, angular rotation
Bluetooth Microcontroller Unit (MCU)
-
Read sensor data, process it, send the data back to the app via Bluetooth
Force Sensitive Resistors (FSRs)
-
Low cost & flexible
-
What can be detected: grip strength, pressure changes over time, contact force patterns
Hardware Cost
IMU sensor = $9
Force sensors = $7
Bluetooth MCU = $5
Buttons + PCB = $3
Battery + charging = $5
Plastic housing = $4
Assembly + packaging = $12
x2
= $88 per set
01 CLINICIAN-FACING APP*
Back in January, Maya and Paulina defined the apple pie goal. Paulina entered it into the system, mapped the required milestones. Since then, she’s been monitoring Maya’s progress through real-time insights from Arlo.
*this is the only screen of the clinician-facing app. All other screens are the patient-facing app.
02 MORNING CALL
Each morning, Arlo greets Maya and reminds her of the 4 milestones she’s working towards that support her overarching goal. Maya needs to be able to hold kitchen tools, stir ingredients, carry her pan into the oven, and lattice the pie crust and top in order to achieve her apple pie goal. She sees today’s list of games along with target areas that they focus on. And finally, she sees a short message of encouragement from Arlo and Paulina before Maya lands on the home screen, ready to start her exercises.
03 START & IN-GAME
Let’s say Maya is ready to play a game. She selects “Restock”, which targets her grip strength and shoulder abduction - a few of the areas she needs to work on to reach her recovery goals. On the game’s intro page, she can see how to play and how her controller interacts with the game. Once she’s feeling ready, she can start playing!
04 GAME RESULTS
After playing the game, Maya sees her results and how she did relative to her milestone progress. Let’s say Maya is really curious about her overall progress though.
05 OVERALL PROGRESS
Maya goes into the progress tab and is able to view all of her progress. She sees how she’s doing overall and how much she has improved over time.
06 MILESTONE PROGRESS
Maya wants more detail on her “carry pan into the oven” milestone. She clicks in and sees an analytical view of her progress. She is able to see minimal functional threshold breakdown on this milestone to fully understand how this milestone can be achieved.
07 BREAKING DOWN MILESTONES
Arlo helps to break down all of this data. For example, Maya wants to know more about her progress in the grip strength threshold. Arlo tells her in Week 1, she had a ~3lb grip strength (meaning she can hold small ingredients for an apple pie like single apples) In Week 2, her grip strength improved to ~5lbs (she can hold small mixing bowls). Arlo links Maya’s progress directly to her apple pie goal, helping her see how each improvement matters. In my research, participants often recognize their progress but don’t always see how it impacts what matters to them. Arlo bridges that gap.
08 BILATERAL COMMUNICATION
Let’s say Maya’s grip strength has improved significantly and her results begin to plateau. Arlo notifies Paulina, who can then adjust Maya’s game difficulty to better match her progress. Paulina can send Maya a message about the game difficulty level update. Arlo ensures easy communication between them, giving Maya low-effort access to her clinician.
06 Benefits & Business Model
BENEFITS
For stroke survivors, Arlo connects clinical progress to personal identity, makes improvements visible and understandable, and builds confidence through milestone framing. For clinicians, Arlo provides detailed insights into each patient’s progress, enabling more precise and personalized recovery plans. Arlo strengths patient engagement and accountability through consistent tracking, reducing unnecessary in-person visits and supports scalable post-discharge monitoring.
BUSINESS MODEL
Clinics subscribe to Arlo to remotely monitor patients and prescribe adaptive rehab, reducing follow-ups and improving recovery efficiency.
Arlo is positioned as a prescription-based clinical tool. It reduces unnecessary follow-up appointments by enabling remote monitoring and adaptive prescriptions. For patients, this lowers long-term costs. For clinicians, it improves care precision. And for insurers, it increases recovery efficiency.
07 Reflections
This was my thesis for Northwestern University’s MS in Engineering Design Innovation program. I put a huge focus on the research side of this project, especially during the first quarter. I remember talking with Jim Wicks, one of my advisors, and telling him how nervous I was to take on the interview and testing process on my own. Listening has always come naturally to me, but I worried about asking the wrong questions, awkward pauses, not making the right connections, or not making participants feel comfortable and safe. I always saw myself more as a designer than a researcher, but this project made me realize that I can be both!
What Went Well
This was my first time finding my own participants to interview and test with, and as a big introvert, I was honestly terrified at first. But, it ended up going really well. Everyone I spoke with was so willing to talk and help me out. I wouldn't have been able to make my design as thoughtful or empathetic without my participants and their stories. I'm so grateful!!!
What Needs Work
I could have improved more in timing out my two quarters better. I had a lot of things that I wanted to do and make, but ultimately did not get to. Because I had so much I wanted to do, I felt myself sacrificing rounds of testing in order to push things towards a higher fidelity for the sake of the final presentation.
What's Next
I learned a lot from this project - about myself and my capabilities, but also about the design field in the medical world. If I were to keep pursuing this project, I would definitely go back and test more before I make a higher fidelity version of my prototypes.
Thesis Studio; guidance from Susan Curtis, Jim Wicks, and Amy Schwartz